

Many people regularly get tested for cholesterol, and the test usually includes other markers and is known as a lipid panel. There’s a lot of confusion about which of these markers are important, so let’s look at the most important lipid panel marker as documented by biomedical science.
What’s a lipid panel?
Lipids are fats, and a lipid panel measures levels of different types of fat in the blood.
More specifically, it measures lipoproteins, which are proteins that transport lipids in the blood.
A lipid panel includes:
- total cholesterol
- LDL cholesterol
- HDL cholesterol
- triglycerides
Up until a few years ago, doctors focused most on total cholesterol.
Now, the focus is more on LDL, the so-called “bad” cholesterol. (A dumb name, but there it is.)
Why the focus on LDL? Most doctors and scientists believe high LDL causes atherosclerosis, which leads to heart attacks.
More importantly, they focus on LDL because there are drugs that lower LDL, and patients must take them for a lifetime. Statins. The pharmaceutical companies coach doctors at conferences, and buy influence via medical journals, to convince medical gatekeepers that they must prescribe statins. “In 2011, US doctors wrote nearly 250 million prescriptions for cholesterol-lowering drugs, creating a US$18.5-billion market”.
However, LDL really doesn’t correlate very well with cardiovascular risk compared to other tests.
LDL cholesterol
First, LDL, the one doctors focus on the most.
In a large cohort of people hospitalized for cardiovascular disease, a total of 136,905 hospitalizations, “almost half have admission LDL levels <100 mg/dL”. Their LDL was normal, yet they had heart disease.
The following graph, put together by Ivor Cummins from data from this study, shows that LDL only matters in the context of low HDL. If you have high HDL, then high LDL is barely a risk factor.
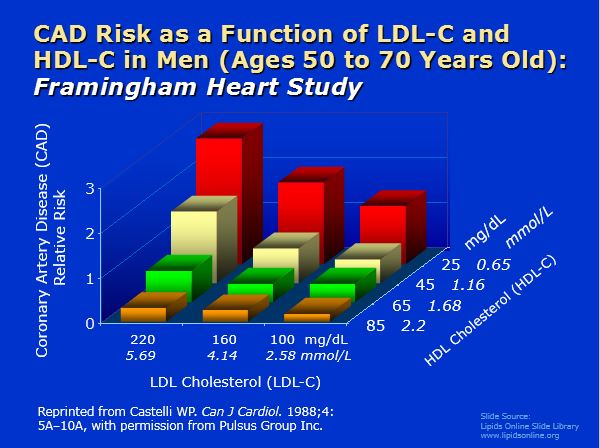
If you have low HDL, however, watch out.
Triglyceride/HDL ratio
The triglyceride/HDL ratio appears to be the most powerful marker for heart disease risk. The lower the better.
Consider the following chart, which I discussed here, and which comes from data from this study.
Those in the top quartile (fourth) of the ratio of triglycerides to HDL had 16 times the risk of heart attack as those in the lowest quartile.

Pretty much explains cardiovascular risk.
This relationship has been found in other studies too.
A high ratio of triglycerides to HDL predicts extensive coronary artery disease. Of all the lipid markers, “only TG/HDL-c and HDL-c were useful for detecting extensive coronary disease, with the former more strongly associated with disease.”
Let me repeat, of all lipid markers, only the triglyceride/HDL ratio and HDL were associated with coronary disease, and the ratio was a stronger marker. No significant relationship was found between total cholesterol or LDL.
“Men with conventional risk factors for IHD have a low risk of IHD if they have low TG–high HDL-C levels.”
The following chart, taken from this paper, shows that men with a low triglycerides/HDL ratio had a low risk of heart disease even when LDL levels were high.

These are of course markers, and not necessarily causative. Raising HDL artifically with drugs has been shown to be ineffective against CVD.
What are good numbers for the triglyceride/HDL ratio?
Last time I checked, mine was 0.5, and it’s hard to get lower than that. Dr. Stephen Sinatra suggests that below 2.0 is ideal.
What does all this mean?
The old model of atherosclerosis and heart disease suggested that arteries were like pipes, and cholesterol clogged them.
In reality, atherosclerosis is an inflammatory disease.
Triglycerides and HDL are markers of insulin resistance, which raises inflammation.
Is there a simple way to identify insulin-resistant individuals at high risk for cardiovascular disease? Yes, a triglyceride/HDL ratio of >3.5 identifies them.
Risk factors for heart disease also raise insulin resistance and inflammation:
- smoking
- obesity
- lack of exercise
- poor diet of processed foods containing sugar and seed oils.
Conclusion
The ratio of triglycerides to HDL is the most important blood lipid marker.
It predicts cardiovascular risk much better than other markers, such as total or LDL cholesterol.






47 Comments
Good article. My trig/HDL ration is .76, which is pretty good (although not as good as yours). My HDL is good also (81). Despite that, my current doctor wanted me to go on statins, because my LDL was 184. That is not going to happen. It’s disappointing and frustrating when most doctors (even some of the younger ones, like mine) are so out of touch with current thinking on heart disease risk (or, the influence of the drug companies is so great that they basically now control what most doctors do). It actually borders on malpractice.
Similar numbers here. Tri/HDL ratio is .88, LDL is 200. Doc already hinting at statins. Not a chance.
Dr’s aren’t nessessarily out of touch as much as they are motivated by the medical profession which unfortunately is driven by the almighty dollar. Follow the money. A man can justified anything if his job depends on it.
Lipids are NOT the best way to measure risk.
CAC is.
Why?
Because calcium dysregulation is the first cause of atheroscerosis.
It begins with microcalcifications which go on to grow to be CAC.
Lipids gone awry follow calcium dysregulation, the first cause.
I would agree. Everyone should get their CAC scores checked. This also emphasizes the importance of magnesium and k2 along with vitamin D.
I know that the CAC test is highly predictive of heart attack risk, but I’m concerned about the exposure to radiation from the test. I know it’s not a huge dose of radiation, but I also get radiation from dental x-rays, etc., and cumulative exposure over ones lifetime is important. My thinking has been that…….with a trig/HDL ratio under 1.0, I don’t think it’s necessary for me to get the CAC test, considering the radiation exposure. I would be interested in your thoughts about that, Paul, Micki, and PD (and others). Thanks in advance for your responses.
Depends how much of your life you’ve had a good ratio for. ; – ) If you’re considering getting it done, ask what the radiation dose is. It apparently ranges from around 1 (about the same as a mammogram) up to 8-10. Also, you could take high dose antioxidants after a scan to try to offset the damage. One suggested cocktail is ascorbic acid, α-lipoic acid, selenomethionine, co-enzyme Q10, and vitamin E – 24 hours after exposure. Note that timing seems to be important. I wish PD Mangan would do an article on this! ; – )
I don’t disagree, but try telling the medical profession that. Patients get lipid panels and rarely CAC.
Exactly, PD. You go to war with the army you have. Virtually everyone over 40 that’s been to a doctor knows their lipid numbers.
If TG/HDL is high, then get a CAC. Likewise, if your waist/hip is high, then get a CAC. If you are diabetic, or “pre-diabetic”, then get a CAC.
Those are all the well-known and well-regarded risk factors for CVD. If you have risk-factors, then (and only then IMHO) follow-up by measuring the disease, which is to say CAC.
Conversely, no risk factors, no need to measure. Save your money and go for a walk. Or hit the gym.
Just saw this. I rest my case. 🙂 No risk factors. She took the CAC anyway — probably because of LDL, even though it’s not a risk factor — came back 0.
https://twitter.com/Tony87505461/status/1003416524177039360
That’s interesting. Total cholesterol of 344 mg/dl (8.9 mmol/L), LDL of 224 mg/dl (5.8 mmol/L), HDL 108 (2.8 mmol), triglycerides 62. Trig/HDL ratio is 0.57. Demonstrating the superiority of the rig/HDL ratio; despite high total and LDL, CAC = 0.
I would generally agree with you but cardiovascular disease remains the number one killer and the risk factors are numerous. These include family history ( even a grandparent), smoking,sedentary life style, even a small elevation in blood pressure. Trig/hdl ratio, BMI over 24, elevated waist to hip ratio. Not to mention that I’ve seen some people have heart attacks with no apparent risk factors at all. The radiation level is very low as is the cost.
I still say that everyone should know their score.
risk factors are numerous
From where I’m sittin’ they may be numerous, but they are correlated out the wazoo.
One thing that probably needs stipulated is which demographic is being discussed. There are three obvious and distinct categories: mainstream clueless; mal-informed; and twit-fit.
With regard to mainstream, you can look at these people and 90% of the time know if they are a heart-attack waiting to happen. IOW, correlated out the wazoo. On the plus side, it’s not uncommon for them to have had some blood work done and the Trig/HDL is a much more reliable factor that they can reference than LDL. From there, sure, spring-board them to a CAC, but I doubt you’re going to convince many of this group they need a CAC unless you can show them their lipids are actually in bad shape.
With regard to mal-informed, well, it’s a toss-up between cancer and heart-attack with these people. Good luck getting through their smug shell. It’s also true that nothing less than a failing CAC will convince them they’re the butt of a conspiracy. But good luck getting them to get one. Maybe if you couch it that it’s something they can “win” and lord over the people in the first group. 😉
With regard to twit-fit, if they are practicing what they preach, the risk factors are again pretty self-evident. Are they fit, and for how long have they been? Does a <50 yo w/ 10+ year history without any of the Big 3/4 risk factors (smoking, obesity, trig/hdl, seed oils) need a CAC? IMHO not really, but it's also true this is a pretty small group: a bunch of cranks, mal-contents, preppers, and more than a few gold-bugs, truth be told.
A 60+ yo? Given that we've been dealing with an active dis-information campaign for 40 years, maybe. I'll grant we're in the "cheap diagnostic with very little downside" case. But on the other hand, what would you do with the information? This person is already with the program. I suppose they could get more religious with their dietary supplements and strength training program, if such is needed, but if they are already on it… what's the point?
Finally, I'll add, 10 years from now, when that 50 yo twit-fitter is 60 — or this 45 yo is 55 😉 — and we have a 20+ year history without any of the Big 4 risk factors I'll stand-by my opinion that the CAC is not needed.
Speaking of correlated factors, this chart comes from the same study that I posted about in the article. It shows risk of coronary disease by Trig/HDL and LDL, among smokers vs non-smokers. This is an astounding chart – smoking hardly even mattered! Similar charts are in the article for hypertension and physical activity: in terms of heart disease, if your trig/HDL ratio is low, you can get away with having lots of other risk factors. Basically, as I see it, insulin resistance trumps everything in terms of heart risk, going by this study at least.
“a bunch of cranks, mal-contents, preppers, and more than a few gold-bugs, truth be told.” – *raises hand*
Insulin resistance is indeed the driver of a lot of chronic diseases. The fasting insulin test is one that people should consider getting more often, IMO. Probably a better test (more informative) than fasting glucose.
Annnnnnd… it’s correlated. 😉
@Micki Jacobs. What is calcium disregulation? Can you point me to any literature on that?
I used to believe that the higher the hdl the better but then came drugs that raised the levels and people had an increase in coronary events. I am always more concerned about total mortality rates than I am in any one disease. This study showed that there is a definite sweet spot when it comes to overall mortality rates and hdl cholesterol levels and that spot is between 35 to 40 mg/ dL and mortality climbs with both high and low levels. Yhttps://www.healio.com/internal-medicine/cardiology/news/online/%7B3136b60b-80a9-4a0f-aa84-9c727d971ed7%7D/high-hdl-cholesterol-levels-linked-to-excessive-mortality
So my triglycerides are about 85 and hdl of 45 when last checked. I used to worry that my hdl was too low, but now I’m okay with it.
Paul, great article you referenced. I enjoyed reading it. The PMID is 28419274, and the full text (link on my name) is free. If you look at the charts, the sweet spot for overall mortality and HDL cholesterol levels is 58-76 mg/dL for men and 77-96 mg/dL for women. In comparison, the adjusted hazard ratio for HDL levels 35-40 are around 1.08 for men and 1.24 for women.
Paul,
Look at the charts in the full study you cited (it’s PMID 28419274 and the full text is free), the sweet spot for overall mortality and HDL cholesterol levels is 58-76 mg/dL for men and 77-96 mg/dL for women. Mortality climbs above and below those levels. The adjusted hazard ratio for HDL levels at 35-40 mg/dL are around 1.08 for men and 1.24 for women.
I take 5 mgs of Crestor EOD – last blood test my trig/HDL ratio was .63
If you normally get your results in mmol/L etc, just be aware you need to convert to US units before calculating the ratios. If you use “rest of the world” numbers you will get a very different numerical result for your ratio, which cannot be compared with the targets mentioned.
Thanks, Dave, that is true. The NIH has a nice conversion factor chart.
Or use differents threshold for mmol/L: “TG/HDL-C ratio less than 0.87 is ideal” from https://www.docsopinion.com/2014/07/17/triglyceride-hdl-ratio/
Yeah. Why is that?
Because mmol is a measure of the concentration of molecules, while mg is a measure of their weight. Since HDL and triglycerides have different weights, comparing mmol is not an apples to apples comparison. If you convert them to equivalent weights, then you can compare the ratio. If the original work had been done using mmol, that would work, but there would be a different normal range.
I wasn’t sure if the studies cited included women. They generally have quite high HDL levels. (at least until menopause), along with low incidence of CVD. Thus, their inclusion could bias these conclusions.
I just checked on my most recent lipid panel. My Trig was 74 and my HDL was 51, for a ratio of 1.45. Do I need to raise my HDL or lower my Trig? Both? How?
Generally, low-carb and no sugar will lower triglycerides, fish oil too. Exercise raises HDL.
Here the TG / HDL ratio is 0.5. But because HDL is too high. It has reached 139. It is rare and does not mean proportional security, that is, above any limit would not have this effect, according to li. Do you know anything about it?
See the study in Paul Rivas’s comment above. You could potentially have a higher all cause mortality from the higher HDL.
Hello PD, this comes in a very good timing.
I am sorry to post this, I know this is not a medicine practice, but I just wanted to share my case, as I am concerned. My lipids have been getting steadily higher since I left vegetarianism and started eating real food and ditched the soya milk, cereals and most of the fruits.
I just had a new lipid panel done and my doctor is concerned about my results:
Cholesterol total 234 * mg/dL (2012 value: 170)
(too high in his opinion)
Cholesterol HDL 99 mg/dL (2012 value: 68)
(the same thing, he says it is not good)
Cholesterol LDL 121 mg/dL (2012 value: 92)
(too high either)
Triglycerides 68 mg/dL (2012 value: 49)
(normal values)
He says that I have to keep track of this.
The rest is just perfect:
Insulin 4,6 μUI/mL
Glucose (suero/plasma) 78 mg/dL (2012 value: 70)
My blood pressure is as always: 6-10, 65 bpm.
The body scan says I have 20% more muscle and 40% less fat than than a healthy woman my age and height.
He says that I should go thought a CAC scan to be sure.
I discussed with him that I do not have any other risk factor: I do not smoke, I exercise…
I would love to have your opinion on this 🙂
Thanks!
Hi Paloma. Basically, your panel is very similar to mine. Your triglyceride/HDL ratio is 0.69 which is excellent. Your insulin and glucose are excellent. And your body composition is excellent. So, I can say that with your lipid panel and other tests similar to mine, I don’t worry about my lipids. I believe that the trig/HDL ratio along with insulin and glucose are the major risk markers. As Dr. Rivas suggests, those that want to go further could get a coronary artery calcium (CAC) test.
Hello PD,
Thanks very much for your answer. I will rather have a CAC test in a couple of years than starting taking statins without any risk factor.
Cheers!
Paloma
Hi Paloma,
While the Trig/HDL ratio might be statically significant, it is not foolproof. I am a perfect example of that fact. I have 20 years of annual bloodwork where my Trig/HDL ratio never exceeded 0.8. While my LDL was always high (120-160), I told myself that all this HDL (75-100) combined with my low Trig (44-80) would keep my arteries relatively free of plaque. Boy was I surprised this last January when I got a CAC score of 768! I’m now on statins.
If you’re running an LDL over 100 then I suggest you get a CAC score and if it’s anything over 100 then you should consider statin therapy. I also suggest that you test your C-reactive protein to learn your overall inflammation level.
BTY
I know of 2 types of heart scans. There’s the standard 64 slice CT scan and there’s the newer EBCT( electron beam CT scan). The former costs $100-$150 and doses you with the normal CT radiation. The EBCT is more expensive ~$300, more accurate (but who cares) and doses you with less radiation.
Hi Chat
I’d be interested to know what was your HbA1c (glycated hemoglobin) throughout this period? This is a very useful marker of longterm oxidative stress when combined with TG/HDL.
I would also like to know your GGT level from a liver panel as a marker of glutathione /oxidative stress?
ChetT (apologies)
P.D.,
Not sure if you’ve seen this but it’s exactly what you’ve been saying..
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0157934
High ferritin and insulin resistance going hand in hand in post menopausal Korean women
Got my donation in today. Here’s to Dumping Iron ??
Thanks, Matt.
Don’t exclude high serum iron…. it’s not just ferritin that is the danger.
On the topic of blood tests, I am a relatively young man, under the age of 35 and soon I want to start a strict, intense 8 week program and at the end reward myself by getting my blood tested and see the results. I am most interested in T levels naturally but would like to know what other things I should look for/ask about.
Only Matt mentions iron (ferritin, actually, though high iron, period, is the issue).
Seems your PS at the end is missed/overlooked, Mr. Mangan:
“PS: High iron is an overlooked risk factor for heart disease and a number of other diseases. Find out why and what you can do about it with my book, Dumping Iron.”
Liked this piece but I am confused…
I am in Canada, and had my lipids screned in June. We use mmol/L
My HDL = 1.04 mmol/L which converts to 40.22 mg/dl
My TG = 1.43 mmol/L which converts to 126.66
Which figures do I use for the ratio? mmol/L gives me a ratio of 1.375.
If I use the mg/dl figures my ratio is 3.15!
Why the disparity? Am I doing the math wrong?
Thanks for some clarification!
-Adam in Toronto
Hi Adam, for this ratio, you must use mg/dl. Assuming you converted correctly – and using this guide, it appears you did – the latter answer is correct.
What if your ratio is really high? Would statins be warranted then?